Percentage of Clinics Experiencing Targeted Intimidation of and Threats Against Doctors and Staff 1993-2022
Feminist Majority Foundation Clinic Violence Survey
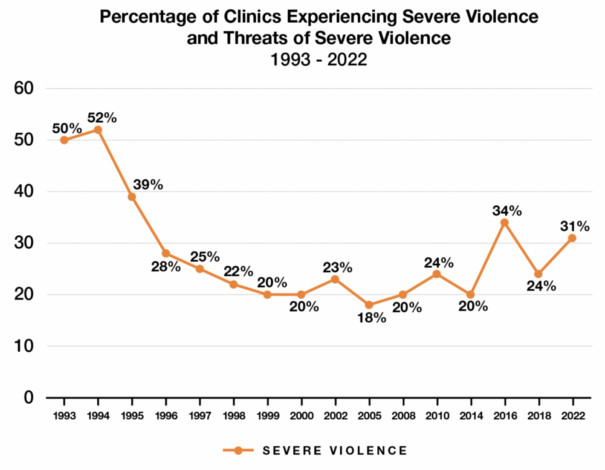
The National Clinic Violence Survey is compiled by the staff of the Feminist Majority Foundation’s National Clinic Access project, measuring anti-abortion violence and harassment. This survey is one of the most comprehensive studies of anti-abortion violence and harassment directed at clinics, patients, health care workers and volunteers in the United States and includes abortion providers of various organizational affiliations as well as independent clinics.
- 2022 Clinic Violence Survey Report
- 2018 Clinic Violence Survey Report
- 2016 Clinic Violence Survey Report
- 2014 Clinic Violence Survey Report
- 2010 Clinic Violence Survey Report
- 2008 Clinic Violence Survey Report
- 2005 Clinic Violence Survey Report
- 2002 Clinic Violence Survey Report
- 2000 Clinic Violence Survey Report
- 1999 Clinic Violence Survey Report
- 1998 Clinic Violence Survey Report
- 1997 Clinic Violence Survey Report
- 1996 Clinic Violence Survey Report
- 1995 Clinic Violence Survey Report
- 1994 Clinic Violence Survey Report
- 1993 Clinic Violence Survey Report